Medicine case
A 55 year old lady from Nalgonda presented to the medical OPD with complaints of distension of abdomen and swelling of lower limbs since 3 months. Self admittedly, a proud mother of 4, the patient was absolutely normal 15 years ago
when one summer's afternoon turned eventful for her, having developed cough with dyspnea and mild expectoration. The cough was occasional but present throughout the day, associated with very little colorless sputum. At the same time she also had dyspnoea and her husband intervened and reported wheeze also. She denies a seasonal or diurnal variation in cough and dyspnea. She also denied chest pain and hemoptysis at any point. The husband however says he noticed her wheezing early in the morning but it never woke her up from her sleep. Interjecting at this point, I ask if there was any exposure to biomass fuel usage and the patient nodded in affirmative, with an exposure to wood smoke for 50 years (until 5 years ago). She denies active or passive smoking. She is unsure of a family history of similar events. These events lasted for 2 years. The couple reported that a consultation with a local general practitioner and therapy prescribed by him resulted in complete cure of her symptoms. This was after several consultations in vain.
13 years ago, the patient developed distension of abdomen with diffuse pain. She says that pedal edema preceded this abdominal distension. At the same time, she also reported early satiety and belching. She never had weight loss or loss of appetite. The patient says that her abdomen was 'tapped and 1.5L of fluid drained' after which she had significant symptomatic relief. She had to revisit the hospital after developing persistent lower abdominal pain with menorrhagia, at which she was diagnosed with fibroid uterus and iron deficiency anemia. 2 packets of blood and a Total abdominal hysterectomy gave her significant relief. She never had to visit a hospital again for the next 12 years.
1 year ago, for a low back ache, she visited the local practitioner. She was diagnosed with diabetes and hypertension and was started on medication.
Since 3 months, the patient developed pedal edema and distention of abdomen again. She also has early satiety. She however, has no pain this time. No history of heartburn, dysphagia, dyspepsia, regurgitation, vomiting, visible bowel movements, no history of chronic hiccups, no history of hematemesis, melena or constipation or loose stools. She hasn't been dyspneic before the distension of abdomen started. She never had palpitations or chest pain or syncopal attacks.
Her pedal edema is associated with brownish discoloration of both feet. She also reports her footwear slipping while walking since the last 6 months. She also has tingling with numbness in her feet. The patient remembers that she can feel the temperature of water on her skin. She feels she can also feel pain. She never reported bowel and bladder abnormalities.
The patient is on a diabetic diet, is well supported by her husband. She is proud of her children and says she holds her head high after having gotten them all married. Her knee pains cause some limitations to her work but she has an otherwise undistressed life with good functional capacity.
Patient also had painful blisters on her left facial region with similar lesions in her left ear. They have now healed but she still has pains.
Family history: no similar complaints in family
Personal history:
Diet : mixed
Appetite: normal
Sleep: adequate
Bowel and bladder movements :regular
No addictions
Drug history: not allergic to any known drugs
General examination: patient is conscious, coherent, cooperative , moderately built and moderately nourished.
Vitals:
Temperature: afebrile
Heart rate: 70 bpm
Respiratory rate: 17/min
Bp: 120/70 Mm Hg
Systemic examination:
Per abdomen:
Inspection:
Abdomen is distended
Umblicus :central
Hernial orifices are free
No scars , engorged veins,sinuses
Palpation:
No local rise of temperature
No tenderness
Splenomegaly is present
Percussion: shifting dullness is absent
CVS examination:
S1 ,S2 heard, no murmurs
CNS examination:
Higher mental functions intact
Tone normal ,power normal
Biceps , triceps, supinator reflexes : 2+in both upper limbs
Knee , ankle reflexes are absent in both lower limbs
Cranial nerves examination : normal
RESPIRATORY SYSTEM examination:
Bilateral air entry present
Normal vesicular breath sounds are heard
The following investigations were done:




















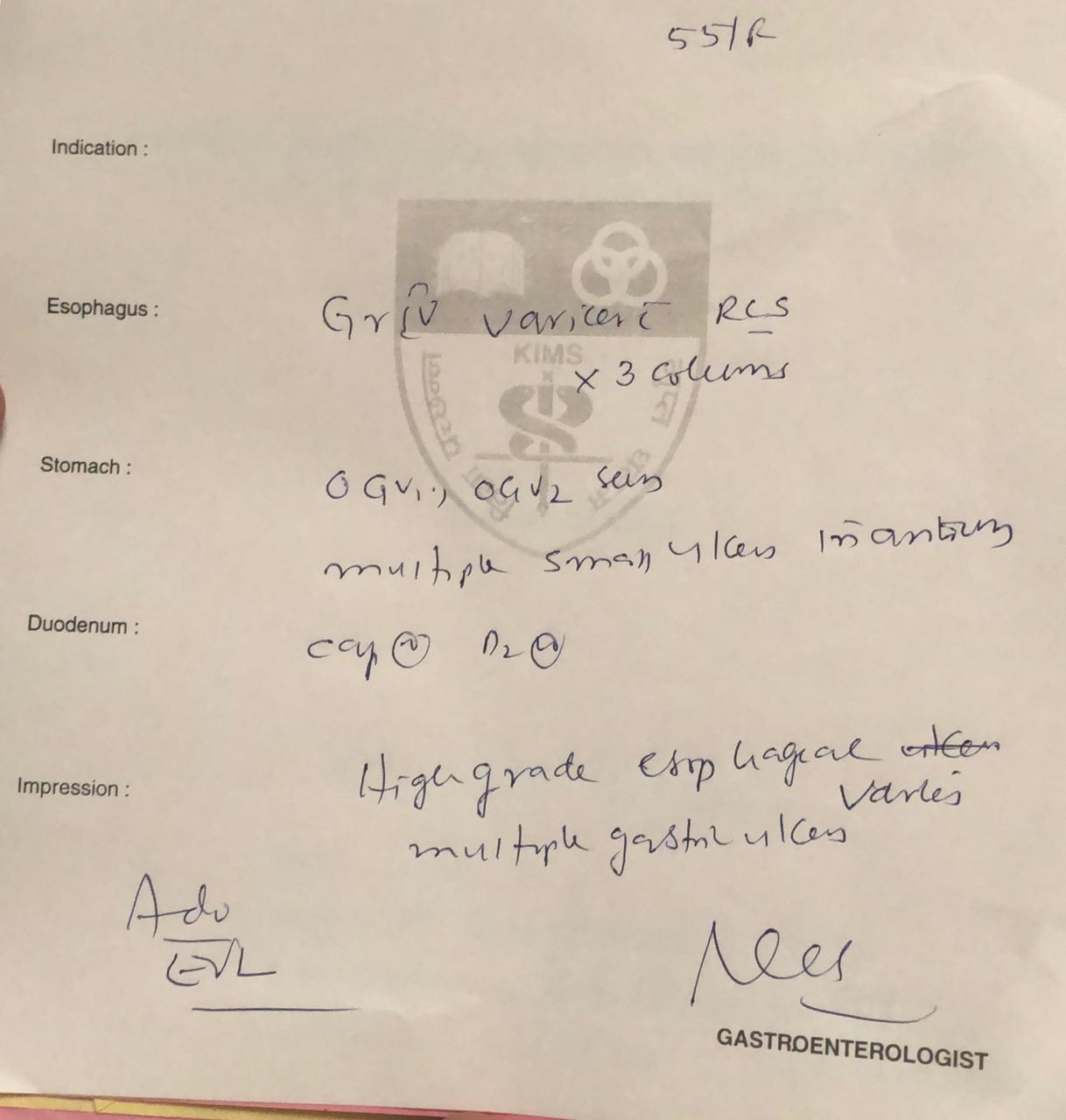
Provisional diagnosis:
1.Extra hepatic portal vein obstruction _portal hypertension with grade 4esophageal varices with massive splenomegaly with NIEC risk index of 37%risk of bleeding at 1year
2.Metabolic syndrome with DM type2,hypertension and abdominal obesity with diabetic neuropathy.
3.left ramsey hunt syndrome
Treatment:
1.T.lasilactone (20/50mg) PO/BD
2.T.Carvedilol 3.125 mg /PO/BD
3.T.Reclimet /PO/OD
4.T.Pregabalin M 75mg/PO/HS
5.T.Brufen/PO/BD
6.T.Acyclovir 200 mg /PO/QID
7.Moisturex soft cream local application twice daily

Comments
Post a Comment